Patients eligible for epilepsy surgery
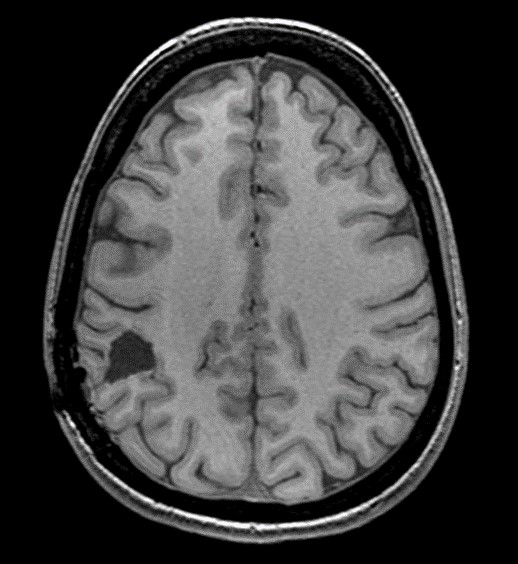
The main surgically curable syndromes are mesiotemporal epilepsy (associated with hippocampal sclerosis) (Figure 1), epilepsy caused by a congenital tumour (known as neurodevelopmental epilepsy) or by a malformation of the cerebral cortex (the most common is focal cortical dysplasia). More rarely involved are vascular malformations (cavernomas) and scarring lesions.

Brain MRI: image of hippocampal sclerosis: atrophy of the left hippocampus (arrow)
Pre-surgical check-up
Potential candidates are selected on the basis of clinical data, EEGs and brain imaging from epilepsy patients undergoing neurological or neuropediatric consultations. Long-term video-EEG recording is usually performed to confirm the focal origin of seizures and correlate it with clinical and imaging data. This initial assessment may be sufficient to establish a surgical indication. It is then complemented by a pre-surgical workup that includes a more specific MRI, with a functional study, coupled with a PET (positron emission tomography) scan, and a neuropsychological workup. In some patients, intracerebral exploration using deep implanted electrodes (SEEG – stereo-electro-encephalography) (figure 2) may be necessary to identify the epileptogenic zone and define the surgical strategy.
Implantation of electrodes for SEEG exploration

Implantation of electrodes for SEEG exploration
Surgical techniques
Surgical techniques have diversified over the last 4 decades, and today combine resection proceduresThese are the most commonly used and adapted to each patient (Figure 3), those of focal destruction (radiosurgery, stereotactic thermocoagulation), those of disconnection (hemispheric or lobar) and those of neuromodulation (deep brain stimulation and vagus nerve stimulation). Functional brain regions are no longer inaccessible to a surgical procedure that is effective on seizures and respects functional structures. Highly epileptogenic lesions, such as focal cortical dysplasia, can be completely resected without unacceptable functional risk and with excellent seizure results.

Surgical resection of right parietal focal cortical dysplasia.
Surgery results
The results of surgery on seizures depend on the etiology of the epilepsy and the quality of the surgical resection. In mesiotemporal epilepsy, 60-80% of patients who undergo surgery can expect to be seizure-free; over 80% after resection of a neurodevelopmental tumor (DNT, ganglioglioma), and almost 90% after resection of focal cortical dysplasia. Long-term seizure suppression is associated with improved quality of life, reduced mortality and fewer side-effects from chronic epilepsy, and drug treatments can be reduced or even stopped in the best cases, not to mention a reduction in the cost of the disease.
Post-operative MRI showing the resection cavity, sufficient for seizure healing.
Outlook
There is still progress to be made in this functional surgery.
The first are organizational, aimed at earlier identification of good candidates for surgery in the epilepsy patient population, and reducing delays in access to pre-surgical assessment and surgery, by creating care networks, particularly during the child-adult transition; they also concern post-operative follow-up, which determines the quality of surgical results.
The second is technological, with advances in preoperative imaging (ultra-high-field MRI), making it possible to identify brain lesions that are invisible on routine imagers; with improvements in surgical techniques (development of less invasive focal techniques that are still effective); with the development of high-resolution surgical imaging methods (fluorescence imaging, OCT, ultrasound), for more precise real-time guidance of the surgical procedure.)
A multidisciplinary activity
Epilepsy surgery is a multi-disciplinary activity, requiring expertise in various fields – neurology, neurosurgery, neurophysiology, neuroanesthesia, neuroimaging, neuropathology – an experienced paramedical and medico-social team – neuropsychologists, EEG technicians, IDEs, social workers – as well as specific architectural and technical equipment – recording rooms and monitoring stations, implantable medical devices -. It is performed in hospitals that have all the skills and equipment on site.
Projet Epiliepsie – Nouveau Lariboisière
With the support of the University of Paris and GHU-Nord, the new Lariboisière hospital project includes epilepsy surgery. It has the environment needed to develop this functional neurosurgery activity, and is committed to recruiting the human skills, training staff and acquiring the equipment essential to the practice of this surgery in all its aspects: quality care, teaching and training, research.