What is the origin of chondrosarcomas?
Chondrosarcoma is a malignant (cancerous) tumor, generally originating in the cartilage cells of the femur, arm, pelvis, knee and spine.
It can also be located in the base of the skull, its origin being the cartilage between the clivus (part of the sphenoid bone) and the petrous bone (= rock, part of the temporal bone). This is known as petroclival synchondrosis.
Although this tumor is considered to be cancerous (histologically), in the skull base it is most often a slowly progressive tumor. However, it can sometimes be aggressive. Its natural history and factors influencing prognosis are imperfectly understood.
Who’s affected?
This is a very rare tumor, accounting for 6% of skull base tumors. In the vast majority of cases, chondrosarcomas are isolated, but can also occur in the context of diseases such as Ollier’s or Paget’s disease.
Most patients are between 30 and 50 years of age, and include both men and women.
What are the symptoms?
This tumor usually develops slowly, and symptoms are usually delayed.
Symptoms are variable and directly related to location. At the base of the skull, the most frequent symptoms are headaches and double vision. Other symptoms may include visual loss, hearing loss, difficulty swallowing, hoarseness, walking problems, motor weakness and more.
How is the diagnosis made?
The tests used to identify tumors are CT scans and, above all, MRIs. The distinctive appearance and localization of chondrosarcomas on CT and MRI scans very often leads to a strong suspicion of this diagnosis.
As this is a rare tumor, radiological diagnosis requires experienced radiologists, and it is sometimes difficult to tell the difference between a chondrosarcoma and a chordoma on imaging.
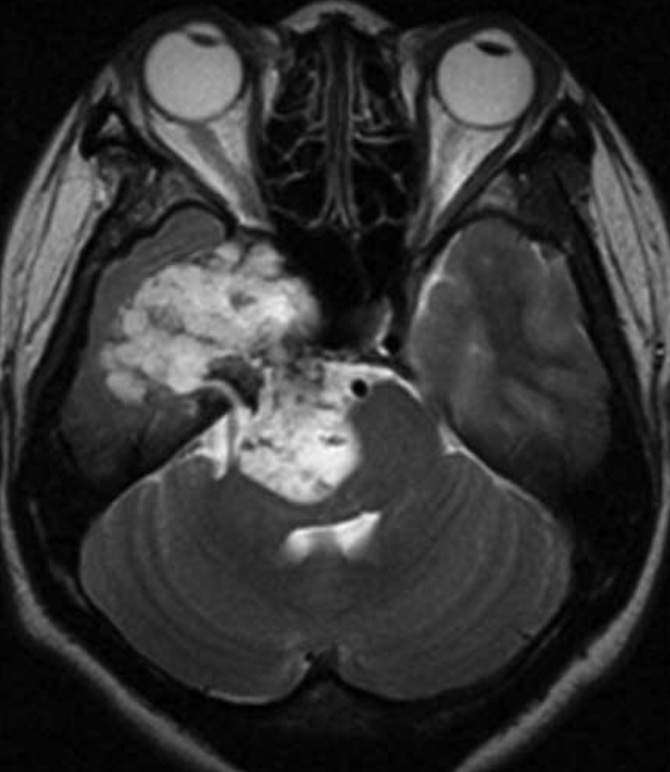
Chondrosarcoma located in the right cavernous sinus, petrous apex and compressing the brainstem.
Definitive diagnosis is made by analyzing the tumor after it has been removed.
Are there different types of chondrosarcoma?
There are several types of chondrosarcoma. A distinction is made between conventional, clear-cell, mesenchymal and dedifferentiated chondrosarcomas. Clear-cell, dedifferentiated chondrosarcomas are exceptional in the skull base. Mesenchymal chondrosarcomas are rare and more aggressive, with a higher risk of recurrence.
Conventional forms are subdivided into grades I, II and III, with grades I and II being the most frequent. The risk of recurrence increases with grade.
What is the treatment?
-
Multidisciplinary approach
A multidisciplinary approach is vital in the management of these lesions.
We collaborate with several teams in the management of these tumors:
– the ENT department at Lariboisière Hospital,
– the Neuroradiology Department at Lariboisière Hospital,
– the Orsay proton therapy department,
– Institut Curie: Dr Hamid Mammar, Dr Valentin Calugaru,
– Gustave Roussy Institute: Dr Stéphanie Bolle.
A national multidisciplinary meeting, attended by all those involved in the care of chondrosarcoma patients, is held every month to discuss patients in need of care or undergoing treatment.
-
Is a biopsy necessary?
A biopsy is rarely necessary. It is sometimes difficult to tell the difference between a chondrosarcoma and a chordoma, so a biopsy can sometimes be used to adapt the surgical strategy.
-
Surgical treatment
Surgery must be performed in centers with experience in skull base neurosurgery.
These are complex injuries to the base of the skull, requiring the mastery of a number of specific surgical techniques.
The aim of surgery is to remove as much of the tumor as possible, while preserving the nerve structures in the immediate vicinity. This is not always possible, particularly at the base of the skull, due to the presence of critical vascular or nervous structures in the immediate vicinity of the tumor, or which cross the tumor. The aim is also to move the tumor away from the normal structures at risk, which are compressed in preparation for radiotherapy.
-
Radiotherapy
The risk of recurrence at 5 years is around 30-40%, but recurrence is often slow, and the risk of recurrence depends on the grade of the tumor. Depending on the degree of resection of the tumor and its grade, surgical treatment may have to be supplemented by high-dose radiotherapy, as these tumors are resistant to radiotherapy. The technique most often used is proton therapy. It is carried out at the Orsay proton therapy center by specialized radiotherapists:
– Dr Hamid Mammar
– Dr Valentin Calugaru
– Dr Stéphanie Bolle
In very specific cases of small tumor residues or localized recurrence, radiosurgery or hypofractionated stereotactic radiotherapy may be proposed.
-
Chemotherapy
In the case of aggressive, recurrent chondrosarcomas that cannot be reoperated, chemotherapy may be considered, but such situations are relatively rare in the skull base region.