The spinal column is made up of vertebrae and intervertebral discs.
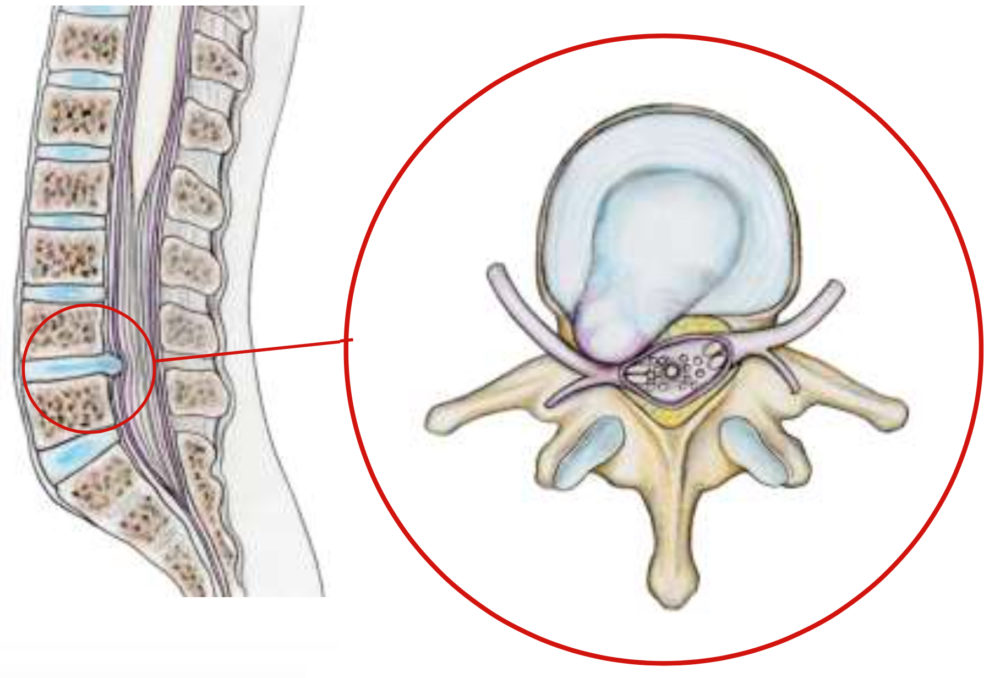
Intervertebral discs are cushions placed between each vertebra, allowing movement by absorbing shocks. They are made up of a fibrous peripheral ring called the annulus and a more gelatinous central part, the nucleus, capable of deforming and resisting compression. This separation between the peripheral and central parts diminishes with age. Under the effect of age, smoking, repeated trauma and genetic factors, the disc becomes fragile and dehydrated. Sometimes, part of the disc migrates through the annulus into the spinal canal, where the dural sac and nerves are located, and compresses one of them. This is known as a herniated disc.
It most often occurs in the lower back, and can lead to compression and inflammation of the lumbar spinal nerves. Pain in the buttock, thigh, leg and foot (sciatica) may be experienced, as well as loss of feeling and weakness, sometimes leading to paralysis.
Surgical treatment is carried out in very specific cases, following a complete assessment and the failure of conservative treatments (medication, physiotherapy, etc.). In the event of extremely intense pain resistant to all analgesics, paralysis or sphincter disorders, emergency surgery may be required. If such symptoms occur, you should seek urgent medical attention.

The symptoms of a herniated disc vary considerably depending on the location of the herniation and your own reaction to the pain. If you have a herniated lumbar disc, you may feel pain radiating from your lower back, down one or both legs and sometimes to your feet (called sciatica). You may feel pain similar to an electric shock.
Activities such as bending, lifting, twisting and sitting can trigger or increase pain. Lying flat on your back with knees bent, or on your side in a “dog-leg” position, can provide relief, as it reduces the pressure exerted on the disc.
Sometimes the pain is accompanied bynumbness and tingling in the leg or foot. It can also be associated with cramps or muscle spasms in the back or leg.
In addition to pain, you may experience muscle weakness in the leg, with a reduction or loss of reflexes in the knee or Achilles tendon. In the case of paralysis, the foot may fall when walking and the toe rubs on the ground. The knee may give way when walking and the leg may give way, leading to a fall. This means that the muscles of the thigh or leg are paralyzed. Likewise, the bladder can become paralyzed, with urine retention followed by urine loss. These are signs of seriousness. If you experience leg weakness or bladder control difficulties, you should seek immediate advice from a neurosurgical department.
The hernia may migrate backwards during a false movement : lifting effort, moving house, violent sporting gestures….. It can also occur spontaneously without any triggering factor. Aging plays an important role. With age, discs dry out and become progressively softer and more pasty. The fibrous outer wall of the disc may weaken, allowing the herniation to migrate. Migration of the herniated disc through the posterior part of the annulus is the cause of back pain, which can be extreme: lumbago with a sensation of “blockage”. Compression of the nerve by the hernia causes pain in the leg.
Genetics, smoking and a number of occupational and recreational activities can lead to early degeneration of the disc.
Herniated discs are more common in people aged between 30 and 40, although middle-aged and older people are at slightly greater risk if they engage in strenuous physical activity.
Lumbar disc herniation is one of the most common causes of lower back pain associated with leg pain. Disc herniations occur less frequently in the cervical region (neck) and much more rarely in the thoracic region in the middle of the back, as this segment of the spine is not very mobile.