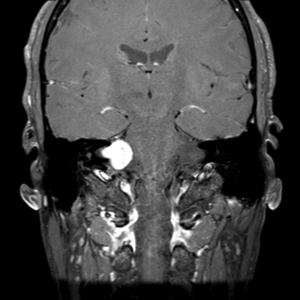
An acoustic neuroma is a benign (non-cancerous) tumor that develops from the sheath of the balance nerves. These 2 nerves link the inner ear to the brain, passing through a narrow canal in the temporal bone at the base of the skull.
These tumors originate within this small bony canal (the internal auditory canal or IAC) and gradually grow out of it towards the brainstem. The brain stem is the part of the central nervous system between the spinal cord and the brain. Once the tumor reaches a certain size, it can compress the brain stem. The brain stem contains all the fibers running from the brain to the spinal cord and back. It is therefore an extremely dense and complex vital structure. In the internal auditory canal where these tumors appear, there are 2 other nerves: the auditory nerve (or cochlear nerve) and the facial nerve. These nerves are also compressed by the tumor.

after Jackler, ATLAS OF SKULL BASE SURGERY & NEUROTOLOGY. Thieme. ©2009
These tumors are caused by damage to the genetic material of the cells that form the sheaths of the balance nerves. The reason why this genetic material is damaged is unknown. No risk factors have been identified.
Acoustic neuromas are very rare. Every year, one acoustic neuroma is diagnosed for every 100,000 inhabitants. They can occur at any age, but are most often identified between the ages of 40 and 60.
The most common symptom is hearing loss. Some people may lose their hearing completely, and sometimes suddenly, but most simply notice a gradual deterioration over time.
Some patients may hear noises or whistling in the ear, known as tinnitus. It can be quite annoying, but there are a number of effective treatments that can help.
Many patients experience occasional or persistent imbalance.
Other symptoms may include numbness of the face, pain in the bone behind the ear, headaches or facial spasms known as “facial tic”. Facial muscle weakness (facial paralysis and facial asymmetry) is unusual.
How fast do acoustic neuromas develop?
Only 40% of vestibular schwannomas increase in size from the moment they are identified. Symptoms permitting, it is therefore important to monitor them before embarking on treatment. As they grow, they generally increase in size slowly, averaging 1-2mm/year, but can sometimes grow faster.
Are acoustic neuromas dangerous?
Acoustic neuromas are not cancers and do not spread to other areas of the body. If they grow, they can compress the cerebellum and brain stem, as well as the nerves around the neuroma. If they develop significantly, they can lead to severe or even life-threatening disorders. In particular, they can lead to dilation of the cerebral ventricles, known as hydrocephalus.
How is the diagnosis made?
Because the symptoms of these tumors resemble those of other middle and inner ear disorders, they can be difficult to diagnose. Initial examinations usually consist of an ear examination and a hearing test. Computed tomography (CT) and magnetic resonance imaging (MRI) confirm the diagnosis and help determine the location and size of the tumour.
- Hearing test (audiometry)
This is a test of hearing function, measuring how well the patient hears sounds and speech. This is usually the first test performed to diagnose an acoustic neuroma. The patient listens to sounds and speech while wearing earphones attached to a machine that records responses and measures hearing function.
-
Auditory evoked potentials (AEP)
detect and measure the conduction velocity of the electrical impulse that crosses the acoustic nerve from the inner ear to the subcortical region of the brain. The patient listens to these sounds while wearing scalp electrodes and headphones. Electrodes capture and record the brain’s response to these sounds. -
MRI
If previous tests show that the patient may have an acoustic neuroma, magnetic resonance imaging (MRI ) is used to confirm the diagnosis and specify the tumour’s characteristics.
What treatments are available?
There are three main ways to treat acoustic neuromas. If the tumor is small, it is often preferable to propose a period of observation to assess its evolution. Unlike other treatment options, it has no potential side effects. However, periodic monitoring is necessary to ensure that the tumor does not grow. If the tumor grows, or if symptoms become bothersome, active treatment is recommended.
Other treatments include surgery and
radiosurgery
. The choice between the two techniques is not always an easy one, and a thorough discussion with your surgeon will enable you to fully understand the advantages and disadvantages of each technique and make the best decision together. These decisions are made in our department during a multidisciplinary
multidisciplinary discussion (RCP Neurinoma)
which bring together neurosurgeons, ENT surgeons, hearing and vertigo specialists, radiotherapists and radiologists.
-
Surgery
Surgery is an effective treatment generally reserved for tumors that have already reached a certain size and for which radiotherapy is not an option. However, the operation is a delicate procedure with the risk of damaging the facial nerve. The result is weakness on the tumor side of the face. Other, less common complications may arise after surgery. Very often, at the time of surgery, hearing is already impaired or very impaired. It is often no longer “useful” because it is dominated by hearing on the opposite side. The chances of preserving hearing when it is already impaired pre-operatively are slim to nil, but the post-operative discomfort caused by this loss is all the more limited if hearing was impaired pre-operatively.
Our team’s philosophy for the surgical treatment of these tumors is to prioritize facial nerve function, even if this means leaving a tumor residue on the facial nerve. a residue is left in around 30% to 40% of our operations. For the majority of patients concerned, this residue does not evolve over time. If this residue is large, it can grow. In this case, radiosurgery is proposed.
-
Radiosurgery
Radiosurgery is an effective treatment, preferentially for small and medium-sized tumors. Radiosurgery involves delivering a high dose of radiation to the tumor in 1 or 3 fractions, using multiple beams that converge at the lesion, with very high ballistic precision. This does not remove the lesion, but it does halt tumor progression. In around 5% of cases, the tumour continues to grow despite treatment. In this case, surgery or a second course of radiation is required. In over 30% of cases, the tumour continues to progress despite effective treatment. This is called pseudo progression. This progression sometimes continues for several years before the tumor shrinks. We must therefore be very cautious before concluding that the treatment was a failure.
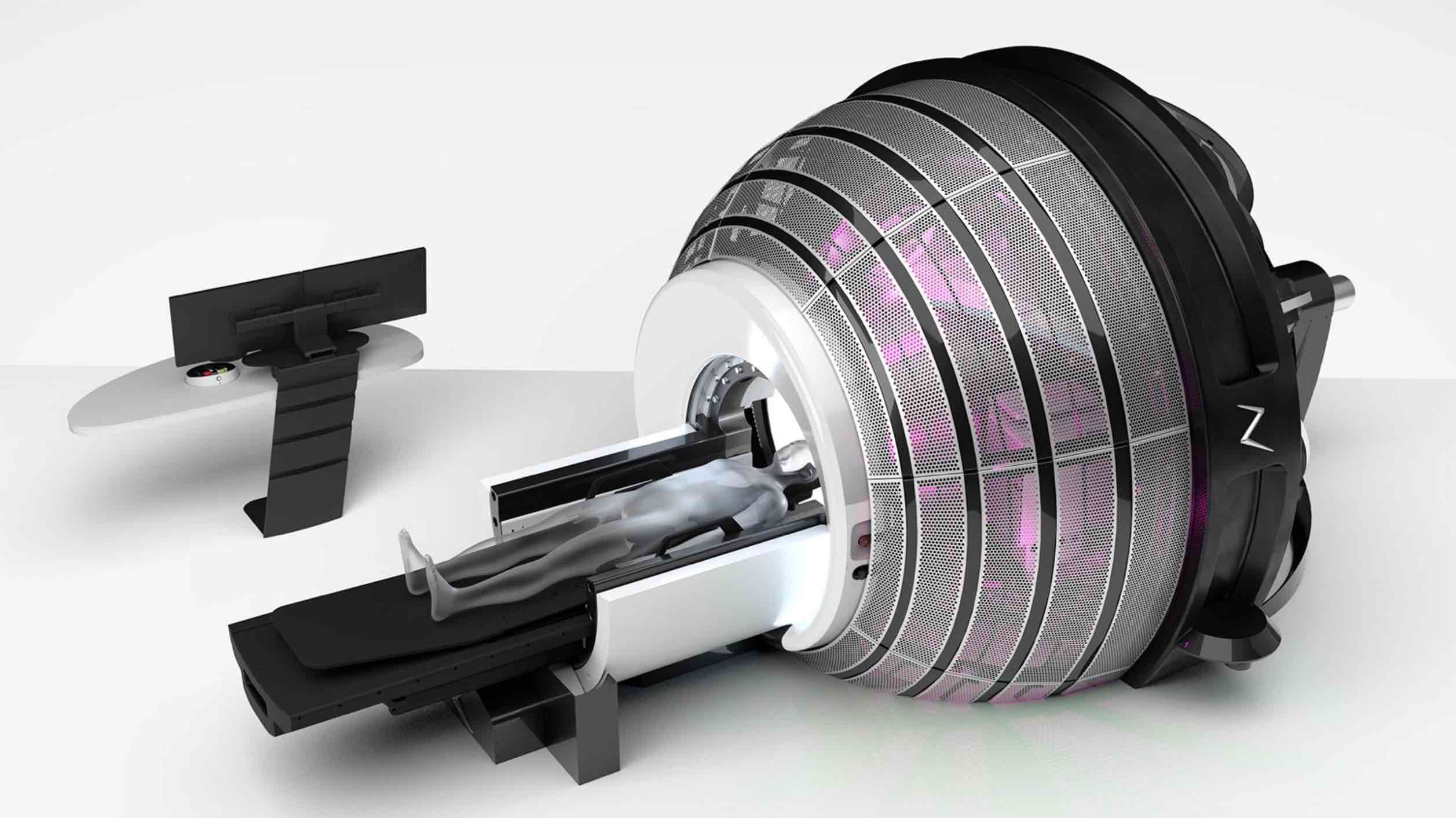
ZAP-X: Radiosurgical device for the treatment of acoustic neuromas or vestibular schwannomas.

Principle of radiosurgery: Multiple beams converge on the target. Each beam delivers a small dose of radiation, but at the target, the convergence of the beams generates a high dose that treats the lesion without damaging adjacent tissue. The precision of the device is therefore crucial, and relies on stereotaxy.
Pluridisciplinary Meeting (RCP) Neuroma
All the teams involved in the management of these tumors (neurosurgeons, ENT surgeons, radiotherapists, neuroradiologists) meet once a month to discuss the cases of patients with neuromas. Together, they define the best strategy for a given patient: surgery, radiotherapy, monitoring.