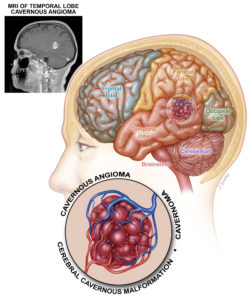
Cavernomas, also known as cavernous angiomas, are small cerebral or medullary vascular malformations that resemble a blackberry. They are made up of small blood compartments, and most commonly grow through iterative microbleeds. They are usually unique, or more rarely associated with multiple other cavernomas in the case of familial cavernomatosis.
There are three main clinical pictures that can reveal a cavernoma: a sudden neurological deficit linked to bleeding in or around the cavernoma, an epileptic seizure (partial or generalized) or a slow neurological deterioration linked to the mass effect of the cavernoma on adjacent cerebral areas.
These clinical manifestations are most often related to bleeding from the cavernoma, its growth or changes in the perilesional microcirculation.
The actuarial risk of bleeding from a cavernoma is around 0.5%/year.
A cavernoma may require treatment, but as its discovery is often fortuitous, it is usually simply monitored. The only recognized curative treatment is surgery, indicated mainly to prevent the risk of rebleeding in the event of repeated hemorrhagic episodes. Once the cavernoma has been completely removed, the risk of bleeding is eliminated. In cases of epilepsy refractory to medical treatment, epilepsy surgery may be proposed to treat the seizures. In deep localizations, in highly functional areas with a high surgical risk, radiosurgery (high-precision, single-session radiotherapy) may be proposed. It does not totally eliminate the risk of bleeding, but significantly reduces it gradually after treatment.